Click to enlarge
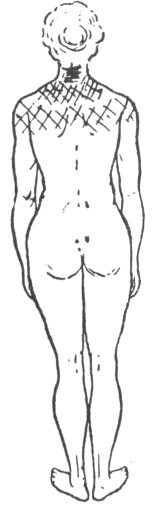
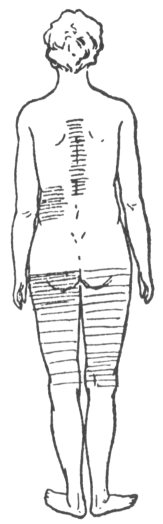
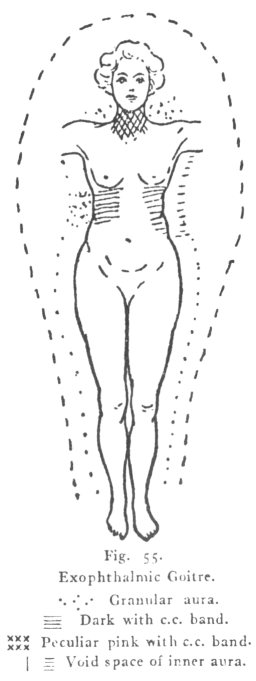
Fig. 55.
Exophthalmic Goitre.
The Human Atmosphere, by Walter J. Kilner, [1920], at sacred-texts.com
THE theory of the complementary coloured bands has already been discussed in a former chapter. There still remains the consideration of the practical use of these bands both in health and disease. Like most other scientific methods of research, a certain amount of proficiency, which only practice can give, is required. After the technique has been mastered with the help of the instructions previously given, there arise difficulties of interpretation. It is essential to acquire rapidity in recognizing the alterations of the tints, not merely to save time, but also to prevent excessive strain upon the eyesight. Immediately after the eyes have been sufficiently (but not too much) colour-fatigued, the first glance is the most sensitive to any slight alteration of the c.c. band, and the more that can be perceived with it the better; later whilst the image is changing colour, rather than when constant, follows the next best opportunity for noticing modifications. The more habitually the band is employed, the more numerous will be the variations recognized. The most that can be hoped for in this chapter, is to give some slight assistance to other workers on this subject, as experience alone can supply the requisite knowledge.
Generally it is inadvisable, even if possible, to examine the whole body minutely at one sitting, especially if it be necessary to employ several complementary colours, as the observer's eyes become fatigued and therefore incapable of appreciating the
slighter differences. Fortunately it is rarely necessary to use all the c.c. bands over the entire body, and the procedure in many examinations may be considerably curtailed, if the history of the patient be sufficiently detailed to direct immediate attention to the actually affected organ or part of the body. Again while the shape and general characteristics of the aura are being investigated, abnormalities may attract notice and point to the position of a derangement that needs investigation by the help of the c.c. bands. The following remarks, unless otherwise stated, refer to the blue c.c. band, as in previous chapters.
The colour of the c.c. band when used vertically upon the thorax and abdomen of healthy men and children will be uniform throughout its whole length, unless there is some irregularity in the pigmentation of the skin. This statement is not always applicable to girls above the age of puberty, and seldom to adult women under the age of fifty, in whom the colour will at one time be evenly distributed throughout, while at another time it will be of a darker shade from a short distance below the umbilicus downwards over the lower part of the abdomen. The region where this change becomes most pronounced is about three inches above the pubes. This modification will be found to coincide with the monthly activities of the sexual organs.
One of three conditions is indicated by a vertical c.c. band monochromatic over the whole of a woman's abdomen: (I) most commonly that the last monthly period finished not less than three or four days previously, or that the next is not to be expected within four or five days; (2) amenorrhœa; (3) pregnancy. At the approach of the menstrual period, the c.c. band will be darkened low down, at first slightly and later as the time draws near more deeply. The colour advances from lighter to darker imperceptibly without any definite line of demarcation, so that a comparison
is best made between distant parts of the band. This gradual deepening of colour is of great importance, as it usually serves to discriminate between an alteration incidental to the natural sexual functions and one that should be ascribed to derangements of the abdominal and pelvic organs.
Darkening of the c.c. band in the lower part of the abdomen from other causes is occasionally an insuperable impediment to calculations relating to menstrual periods. Allowance for the pigmentation on this part of the body may sometimes have to be made if the patient has already been a mother, but generally there is no difficulty of any consequence when proper care has been exercised. An interesting instance connected with this subject is that of a women thirty-three years of age, who manifested an incipient darkening of the c.c. band just above the pubes. When informed that she might expect her next monthly period within the following six or seven days, she replied that it was not due for a fortnight. However, at our next meeting she suddenly exclaimed, "do you remember telling me that my monthly courses would take place in about a week? Well, they did seven days afterwards, being a week sooner than anticipated." In another instance a young woman expected to menstruate within three or four days. With her there was no change in the colour of the band above the pubes. It eventually turned out that her period was delayed for a week.
The acquisition of such information concerning the sexual functions is generally unimportant and obtained while other observations are being made, because during the same projection of the band, all modifications of colour in different parts of its length and their limits can be ascertained, and it can also be noted whether the changes be gradual or abrupt, and the line of demarcation sharp. The band will be found wide enough in most cases for the observer to
determine any differences in colour which may happen to occur on the two lateral halves of the body, and to note roughly their position. Subsequently the transverse band should be employed to verify all minutiæ. This latter band has the advantage over the vertical, that during the greater part of the inspection the central portion only need be used, making it easier to watch and freer from errors of observation than when the ends have to be used. Cases 49 and 71, figs. 43 and 56, are instructive and will serve as examples. In the first case when the c.c. band was employed vertically down the middle of the thorax and abdomen, the left side of the former was seen to be lighter than the right for a considerable distance and the upper margin of the discoloured portion lay on the superior aspect of the mamma, while the inferior border was over the lower part of the sternum. The line of demarcation was sharp, corresponding to the median line of the body. Lower down, the band on the abdomen disclosed a small patch of a different shade on the extreme right edge a little above the level of the umbilicus. This gave a useful indication for further investigation with the c.c. band transversely, the result of which has been described elsewhere.
When the examiner begins to scrutinize the spinal column with the c.c. bands he will find it advantageous to divide the inspection into parts, as the band is rarely sufficiently long to cover the whole space simultaneously. Before commencing it will be prudent to take particular notice of the colour of the skin over the vertebral spines, where it has frequently a different tint from the neighbouring portions of the epidermis. This may be a natural pigmentation, or an alteration in colour produced by constant pressure of the clothes. Directly the observer looks at the spine, he will most likely detect some variation in the shade of the c.c. band should derangement be present. The commonest irregularity exhibited on the back are
patches seen on the spine itself, either lighter, darker, or of a different colour as the case may be. These spots may be situated on any part throughout its length, but most frequently over the two lowest lumbar vertebræ and the sacrum in women, where the colour of the band is constantly altered. The reason for this has already been stated. Two other common positions are over the lower dorsal and upper lumbar vertebræ, and over the seventh cervical and higher dorsal spines. Here, usually, some shade of yellow, or else a paler tint of the c.c. band is generally seen, but over the sacrum the shade is dark or the colour often approaches ochre. It is not uncommon to find two or more different coloured patches on the same patient. Another fairly frequent abnormality is the appearance of a coloured streak by the side of the spinal column, while the aura over the spine itself remains natural.
Such spots are invariably attended with pain or tenderness, not necessarily just at the time of inspection, as even weeks may elapse before pain-marks disappear finally. Of this occurrence a good example has been mentioned on page 240. A patch on or near the spine of a light yellow colour, or of a lighter tint than the rest of the band, is a sign that there is no organic mischief, and almost always that the cause is only temporary, not seldom having a nervous origin. The darker patches and those in which the colour tends to ochre seem to point to more important or prolonged disorders.
The next case is of interest as an illustration of the remarks just made and also showing a hysterical type of aura.
Case 70. (Fig. 55.) S., a married woman twenty-eight years of age, childless, complained of vomiting during the previous six weeks, which was increased by any worry, was first examined in 1910.
For three months she had been losing flesh. Her
menses were regular. She suffered occasionally from globus hystericus. Her thorax was peculiar in shape, being straight down, and the sternal notch was as high as the nipples, although her breasts were not pendulous. There was tenderness in the epigastrium, and pressure there induced pain
Click to enlarge Fig. 55. Exophthalmic Goitre. |
showed close to and parallel with the spine, a strip on the left side lighter in colour, reaching from the third to the ninth dorsal vertebræ, having all its margins distinctly defined. This was considered to be a case of nervous vomiting and was treated accordingly.
She was lost sight of for three years as she had left London, but later she returned with a new set of symptoms. She had remained in good health for two years without a recurrence of her old complaint. For the last five or six months, however, she had been getting thin, and at the time of examination she only weighed six stones, seven pounds. All her new symptoms pointed to exophthalmic goitre—slight enlargement of the thyroid gland—prominence of the eyes, especially the left, sufficient for her friends to remark upon, rapidity of the pulse and palpitation, often when in bed, debility and nervousness, tremors of the limbs, particularly of the right hand and leg, strange sensations in various parts of the body. She had also pain in the right side of the thorax, culminating at the tip of the eleventh rib.
Inspection showed both auras to be distinct. The measurements of the outer were identical with those obtained at a former examination. The inner had the same width as before, and was striated over most of the body except by the right side of the thorax and over the sacrum, where it was coarsely granular. On the left side of the thorax it had disappeared close to the body leaving a void space about half an inch in breadth. On both sides of the neck, more especially the right, it was finely granular. The c.c. band revealed a dark patch on the spine between the fifth and the ninth dorsal vertebræ, another over the sacrum, whilst in front there was a third over the right lower ribs. All these places were tender. The extensions by the sides of the neck had a deeper shade than elsewhere.
It will be interesting to compare this patient with
another woman who had been afflicted with Graves' disease for some years, and had been under treatment at different hospitals.
Case 71. (Figs. 56 to 58.) K., a woman thirty-seven years of age, the mother of two children, was
Figs. 56, 57, and 58.
Exophthalmic Goitre.
inspected in 1911. Until marriage she was delicate but had never exhibited any signs of hysteria. Between four and five years ago her illness was diagnosed as exophthalmic goitre. At the time of examination her symptoms were: slight enlargement of the thyroid gland, protruding eyes, pulse fairly normal, no palpitations, and great nervousness. She did not feel so
strong as she did a short time previously, and was depressed. A week before examination a severe thunderstorm frightened her, and immediately afterwards she felt a peculiar sensation in her thighs and legs, the left thigh being the worst. This singular impression continued several weeks before it entirely vanished.
Her aura was a blue grey in colour, and of good size and shape. The outer aura was nine inches by the head and trunk, diminishing to three by the ankles. A side view showed it to be five inches in front, seven at the back with no bulge, and by the legs three inches wide. It was coarsely striated by the neck on the right side, and to a less extent on the left. By the lower part of the thorax on the left side it was coarsely granular, otherwise striation was natural over the whole body. As the woman was standing sideways, a ray was seen proceeding from the twelfth dorsal vertebra. This ray caused a dark patch when examined with the c.c. band. Later on during the investigation the ray vanished, and the place was examined a second time with the c.c. band, when the dark patch was found to have completely disappeared. This is conclusive evidence that a ray and a patch may have a common underlying cause. In addition there was a large dark area over the lower lumbar vertebræ and the upper part of the sacrum. In front the band exhibited a light spot over the left hypochondrium. The band was much deeper in shade over the thighs and legs, being darkest in the places where the sensations reached their maximum. The shading in the figures is proportional to the depth of colour.
She was inspected a second time in the following February. Although the lower limbs were free from the peculiar sensations, the right side of the thorax was now attacked.
Neither aura showed any alteration in size or shape since the previous investigation. However, the c.c.
band was darkened all over the right side of the thorax. The inner lines of demarcation between the normal and abnormal colours were the vertical lines back and front. The left thigh was still deepened by the c.c. band but not to the same extent as before. This was evidently a continuation of the former condition.
Shortly after this examination the patient became pregnant, and while in that state her health improved greatly. In October, 1912, she was inspected a third time. The only change in the shape of her was, as might be expected, in front of her abdomen. Here the outer aura was seven and a half inches, while the inner was three and a half; both were conical. In this case pregnancy caused the outer aura to be diminished in distinctness to a slight extent, while the inner aura was more affected, and had lost much of its clearness. Striation was only to be detected with difficulty. Late in December she gave birth to a healthy girl; both mother and daughter did well. Soon afterwards she removed to another neighbourhood.
With our present imperfect means of investigation, the observer must not expect to see discolouration of the c.c. band over every painful or tender place of which the patient complains. Some of these patches are so distinct that a very cursory glance will detect them, while others differ from the rest of the c.c. bands so slightly that keen sight and a trained eye are required to isolate them. As practice makes perfect, a larger number of these discoloured patches will be discovered.
It is by no means easy to understand why some local disturbances should induce sufficient change in the aura to produce a chromatic alteration in the c.c. bands, while others seemingly similar in every respect give negative results. Intensity of the disorder, especially if acute, appears to be one of the chief factors in the auric change. It is instructive to notice
that these discoloured spots in the c.c. bands projected upon the spinal column are not nearly as common among males as females, and are especially marked amongst hysterical, nervous, and excitable girls and women.
As soon as the examination by means of the c.c. bands, when used vertically, has been concluded, having noted as far as possible the positions of local abnormalities, the transverse band will complete all the information to be gleaned by this method. It will enable the investigator to examine the two sides of the body, and with the same projection to observe if one of the extensions has been affected. As a rule the band will be found wide enough to include the whole of the disordered area, but occasionally further observations will be needed. This is, too, the best opportunity for ascertaining whether a discoloured patch spreads over the whole breadth of the body, or only over a portion, also to determine whether it is situated, in toto, on one side of the median line, or crosses it, or whether again it is only a small spot surrounded by the unaltered c.c. band. A large area chronically affected has usually a deep hue, but exceptions are by no means rare. For examples see cases 49 and 69. Although large patches may be discovered on any part of the body, yet they occur more frequently in some positions than in others. A common situation is over tie hypochondriac and epigastric regions. The following is a good illustration and demonstrates the length of time an alteration may endure, as the period between the first and last inspections was more than five years.
Case 72. A childless woman who had been married several years suffered for more than twelve months with pain in the stomach, which increased after a meal and was often relieved only by vomiting. She was constantly sick, had pyrosis, but no hæmatemesis. Dread of pain, which she described as agonizing,
prevented her from taking any proper food; consequently she was emaciated, weak, and anæmic. From these and other symptoms an ulcer of the stomach was diagnosed, and under treatment she gradually improved and became convalescent. When first examined in 1909, her aura was blue in colour, over eight inches by the head and by the sides of the trunk, and four by the legs. In front it was four inches wide, and at the back nearly six in the lumbar regions, coming straight down. The shape was good. The inner aura was two and a half inches in breadth. There were several rays projected from different parts of her body, one from each shoulder, one from each flank, and on the right side one streaming downwards. As she stood sideways, a sixth was noticed emitted from the lower lumbar vertebræ upwards and outwards. The c.c. band disclosed no patches on the back. In front a dark spot over the epigastrium was present, with its upper border on the sterno-xiphoid plane, and the lower two inches above the umbilicus; the inner margin was at the middle line, and the outer edge on the side of the trunk. This area was several shades darker than the rest of the band, and the left extension was darker than the right.
Unfortunately, after being apparently well for some months, she had a relapse in January, 1910, and as proper attention could not be obtained at home, she entered a hospital for treatment. Finally she was discharged cured, as she had lost all pain, and was able to eat solid food without discomfort. Shortly after her return home she was again examined. There was no difference in the outer aura, but the inner was granular on the lest side from the nipple line to the crest of the ilium, front, back, and side. When the transverse c.c. band was used over this part of the body, the large discoloured patch could be distinctly seen, but was not perhaps quite as plain as it had been
previously. The extension still remained darker than on the right side.
There were two discoloured patches on the back, one by the right side of the third and fourth dorsal vertebræ, where she had previously suffered pain. The second spot was over the lower lumbar vertebræ. The writer thinks these patches may have been present at the first examination, only that not being as proficient with the c.c. bands as later on, he missed them.
In 1914, her aura was inspected a third time. There had been no recurrence of any symptom of ulcer. Although in fair health she had never completely regained her full strength, and just lately had been feeling run down. The size and shape of the auras remained unchanged. By the lower ribs on the left side there was a void space between the inner aura and the body, but lineation in the constricted portion could be distinguished. With the c.c. band the same dark patch over the epigastrium was still in existence, but it had altered inasmuch as the dark portion had lessened in width, and the upper part had become lighter in colour. This was one of the few instances that have been seen of a dark spot turning paler, and the change was exceedingly interesting as being probably the first step towards complete disappearance.
Another example in regard to which it would be superfluous to enter into details as it is so like the preceeding one, is that of an unmarried woman twenty-nine years of age, who was brought by Dr. Merrick. Examination with the c.c. band showed that the abdominal area affected was almost identical with that of the last case, but there was one important difference, viz, that the colour of the patch was lighter instead of being darker than the remainder of the band. Experience having taught that pale coloured spots are generally indicative of temporary disorder, the opinion was expressed that the patient's
ailment was slight and fleeting, which turned out to be correct. A word of explanation is necessary. The writer had intentionally not investigated this case in the ordinary manner, as this had been done by Dr. Merrick, and it was looked upon as a test of the value of the auric changes.
These two are instructive cases in which the c.c. band gave directly opposite colour effects, although the regions under observation were the same in both instances. In the latter example, whatever the malady may have been, there was in all probability a nervous element at work, and very likely the derangement was entirely functional. In the former case the woman was suffering from chronic gastritis with the corresponding tissue alterations.
Analogous changes may occur over the right hypochondrium and are generally also bounded by the middle line of the body. The upper edge is usually somewhere about the level of the sterno-xiphoid plane, while the lower boundary is about the level of the costal plane. These limits are only approximate, and variations constantly occur. When a patch is seen in this position an invarible accompaniment is tenderness of the liver, with or without superficial hyperæsthesia. Persons addicted to imbibing too much alcohol almost without exception show this patch, which in such cases is dark, and generally associated with another discoloured spot over the epigastrium. These two patches may join and make a single large one. Occasionally when the c.c. band exhibits the large dark patch just mentioned, a small area still darker or one of a different tint may be seen within it. Such a small dark spot is invariably of serious import, through which the presence of malignant disease, before it could have been detected by ordinary means, has been discovered, the diagnosis, unfortunately for the patient, turning out to be only too correct.
Case 73. (Fig. 59). I., a married woman sixty-four years of age, who had always been delicate, had her breast removed in 1901. She was gouty and for five years had been a martyr to neuralgia of the face and neck, the sequel of herpes zoster. In December,
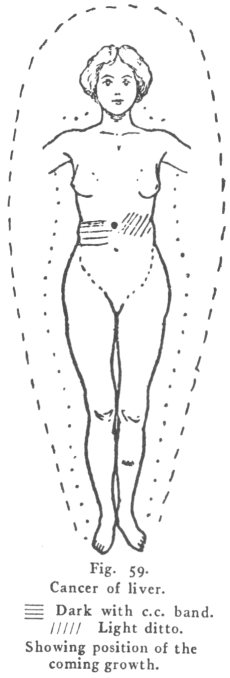 Click to enlarge Fig. 59. Cancer of liver. |
in good health, was two and a half inches wide all over the body and faintly striated. The c.c. band was uniform over the whole body, except in front on the right side, from the pyloric plane to the level of the umbilicus where there was a dark patch, limited by the median line, whilst to tilt right it went as far as could be seen. There was a still darker spot just over the ninth costal cartilage. Over the epigastrium the c.c. band exhibited a light coloured patch. A diagnosis of growth near the gall bladder was made.
She improved for a short time and went into the country for change of air. At the end of May, 1912, she returned home as she had suddenly developed jaundice. Examination of the abdomen disclosed a hard tumour about the size of a pigeon's egg, which could be felt near the gall bladder, exactly in the place where the very dark spot had been previously seen. The tumour grew rapidly, and other nodules soon made their appearance. She survived only five months.
As an antithesis to this case, a woman asked to have her mother inspected as she had cancer of the liver.
Case 74. N., a woman, seventy-three years of age, was examined in December, 1914, without a single question being asked. The colour of her aura looked a greenish blue with an admixture of white—an uncommon appearance. The outer aura was quite up to the average in distinctness, and of a good shape. It was nine inches round the head and eight by the trunk, and four by the ankles. In front it was four inches, and at the back seven at the widest place. The inner aura did not reach the standard of clearness for health, but striation could with a little difficulty be distinguished, and in no place did it exhibit the slightest sign of being granular. When the c.c. band was employed upon the back, a small patch was
perceived on the left side, by, but over, the third and fourth dorsal vertebrae, slightly darker than the rest of the band. In front there was only one faint patch about two and a half inches by two, just over the gall bladder. The other c.c. bands did not assist in any way.
Taking into consideration that the aura was healthy, and that the changes disclosed by the c.c. bands were insignificant, the writer felt confident there was no malignant growth. Palpation revealed the presence of gall stones. The patient then gave the following history: she had been suffering from bouts of sickness for several years, and had been growing thinner for three. There had been pain and tenderness over the gall bladder. Two years previously she had entered a hospital, when an operation was recommended, she believed, for gall stones. She would not allow it to be performed, being timid on account of her age. As a result of the examination she was advised to go at once and consult a surgeon. In this instance the aura did not disclose any facts that could not have been ascertained quite easily by ordinary methods of examination, but it is none the less interesting on that account.
Examination of their aura has been the means of reassuring not a few people who had come up under the impression that they were suffering from cancer.
Another common situation for a discoloured patch is over one and sometimes both groins in women mostly over twenty-five years of age. In no instance has a patch over one groin only of a man been recorded, but in a few cases there have been found dark bands stretching right across the lowest part of the abdomen. The upper margins rarely reach as high as the anterior superior spines of the ilium.
The colour of these patches may be either darker, lighter, or of a different hue, to the remainder of the c.c. band, and if there be two patches, one in
either groin, they are seldom of the same shade, but should they join and form a complete belt across the lowest part of the abdomen, then the colour will generally be uniform throughout its whole length. After tabulating the different cases it was found that sixty per cent. of these discoloured areas were on the left side, about five and twenty on the right, and the remainder on the two sides, while of these latter about half were joined in the centre.
These patches are invariably diagnostic of pain or tenderness, and according to the depth of shade these symptoms vary in intensity. They are usually accompanied by discoloured places on other parts of the body. Their position in women is sufficient to make it probable that they may have some connection with the genital organs, and, if so, are more commonly than not associated with activity or functional disturbance of the ovaries. From this point of view the next case is very instructive.
Case 75. Mrs. N., forty years of age, had her aura inspected during the autumn of 1918. The outer aura was proportionately rather narrow round the head; otherwise it was of good shape, and exhibited no abnormality. It was nine inches round the head, ten and a half by the trunk, six by the thighs, four and a half by the ankles, and the same width at the back opposite the shoulders and nates, coming down straight behind from the head to the feet. Striation of the inner aura was visible all over the body, but by the left side of the trunk and at the small of the back it was coarse. Neither aura quite reached the proper standard of distinctness for a perfectly healthy person. With the c.c. band, a dark patch was observed upon the sacrum, and in front there was one in either groin. The one on the right side extended nearly as high as the crest of the ilium and continued downwards but with lessened depth of colour to the middle of the thigh. On the
left groin the spot was smaller and not so plain, and there was no darkening of the band on the thigh. Besides these she presented other discoloured areas, one by the left side of the dorsal vertebræ, another on the epigastrium, and a third over the right hypochondrium. These may be neglected, being unimportant for the present purpose. In addition to the outer aura which is universal after a person has been electrified, the inner aura by the lower part of the right side of the abdomen and the thigh became augmented.
The patient was a childless married woman who had never been really strong, but who had never suffered from any serious illness. The marked difference in the size and shade of the patches seen with the c.c. band was suggestive of more disturbance on the right side than on the left during menstruation. On being asked whether she suffered an equal amount of discomfort at each period, the following facts were elicited. She had only menstruated a few times in her life, but each month she experienced a considerable amount of pain which was more intense every other time. On the occasions when she had the severer pain, the right thigh always participated in the discomfort as far down as the middle. The lower part of the back always ached.
The alternating violence of the menstrual prodromata points to ovulation taking place successively first in one ovary and then in the other, and more intense functional disturbance when the right was involved.
A discoloured area is of common occurrence over the epigastrium, both in males and females, so common indeed as to seem almost physiological, in the majority of cases where there seems no sufficient reason for suspecting any abnormality. These spots are always light in colour, or of a pale yellow, and are mostly of a fleeting character. The darker shades and hues
denote true gastric derangements of some description. Should the light coloured patches prove to be physiological, they are the only known instances, but the only possible alternative is, that a pathological change so slight as to be imperceptible both to the patient and the observer, exists.
Besides these large affected areas, small discoloured spots may be visible which are usually indications of purely local disturbance, and are accompanied by pain or tenderness. These small areas are frequently coloured, yellow of some shade being the most common, and next in frequency a pinkish tinge, which as a rule denotes a more severe disorder. The greater number of them are completely isolated, but may be included within a larger patch, when they point to a focus of considerable mischief. All parts of the body are liable to them, and position may sometimes determine their importance.
A striking example of the foregoing observations was seen in the following incident. Dr. Merrick, wishing to see the aura, brought a patient with him for examination. Knowing that this woman was suffering from ulcer of the stomach, the writer stated that it was extremely probable that the most painful spot or the position of the ulcer could be detected by the help of the c.c. band. No question was asked. Dr. Merrick was able to see the aura distinctly but not the coloured spot, as he was not accustomed to the use of these bands, and could not keep them fixed on the right place.
Case 76. T., a married woman thirty-three years of age, had been suffering from ulcer of the stomach for a long time. She had already been in a hospital and was advised to re-enter for an operation as she was greatly emaciated, and bloodless as a result of repeated vomiting and hæmatemesis. Her aura was well marked and of a bluish colour. A yellow spot about the size of a shilling was visible by the aid of
the c.c. band on the left side two and a half inches from the median line, and a little below the ensiform cartilage. This coincided with the most painful place, and was so tender that the patient would hardly allow it to be touched. The rest of the epigastrium was sensitive but not nearly to the same extent. Further examination could not then be made. It was curious that no large discoloured patch, as might have been expected, could be seen.
During March, 1910, she was again inspected. She had not been to a hospital as advised, but had, however, improved greatly, having gained weight although still remaining anæmic. Most of the pain had disappeared and only a slight tenderness in the epigastrium persisted, vomiting had ceased, and she was able to eat ordinary food. Some little pain and tenderness still continued in the lower part of the right hypochondrium. Her outer aura measured nine inches round the head and by the sides of the trunk, and gradually contracted to four by the lower limbs. A side view showed the aura extending four inches in front of the body, while at the back it was seven inches in the lumbar regions. The inner aura was two and a half inches all over the body. Through the dark carmine screen this aura looked granular on the left side between the line of the nipples and the crest of the ilium, and when viewed sideways, the same effect was noticeable over the thorax, which was lighter in shade. The change commenced at the median line of the body, the upper margin being at the level of the mid-point of the sternum, and the lower following the outline of the costal cartilages. In this patch there was a still lighter spot coinciding with the yellow one seen at the first inspection. The second discoloured place consisted of a small mark on the right side where the aura was granular.
Occasionally a patient may have considerable bodily disturbance, and yet the aura may be only
slightly involved. As an illustration the following example has been selected.
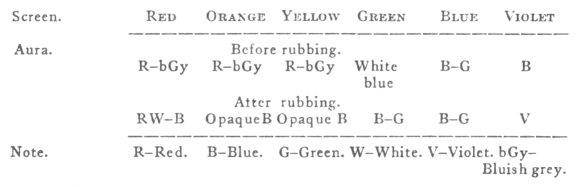
Case 77. (Figs. 60 and 61.) S., a bright sturdy woman, twenty-seven years of age, was inspected at the end of 1913. Twelve months previously she had
Figs. 60 and 61.
Raynaud's disease.
lost her mother after a short illness, the shock of which, together with the extra cares of the house and the charge of a motherless child, produced a slight breakdown. For nearly a year the lower part of the face, the neck, and the upper portion of the trunk constantly turned a very deep crimson, and below this
region in front to the level of the inferior borders of the mammæ, and not quite as low down at the hack, the red tinge was well marked but not to the same extent. The deeper colour had an irregular outline, and the limits and comparative depths are shown in figs. 60 and 61. A phenomenon corresponding to tache cerebrale could be obtained over the whole of that part of the body which was affected. The attacks occurred at any time, whether the woman was alone or with company. A slight change of temperature was sufficient to excite an onset. Each paroxysm only lasted a few minutes, but the average was between twenty and thirty per diem. When flushing, she felt a burning sensation but no absolute pain. The skin over the most affected area was scaly, and over the remaining portion where the tache cerebrale could be induced was dry, being elsewhere normal. The case was considered to be allied to Raynauds' disease, and an exceptional interesting aura, especially with the c.c. bands was expected, but nothing of the kind was found.
Both auras attained the usual standard of distinctness and had a blue grey colour, and were normal in shape. The outer aura was eight inches round the head and by the sides of the trunk, while in front it was four, and behind at the shoulders and nates it had the same width, descending without any bulge. The inner aura was three inches all over the body, with well marked striation, except just above the shoulders where it was granular. Contrary to expectation when there was no flush the c.c. band was even over the whole body with the exception of a small dark patch on the third and fourth cervical vertebræ.
Case 78. A second case showing a very similar condition came up for examination in December, 1914. The patient was a young woman who had never been robust, and at the time of inspection was anæmic,
[paragraph continues] For some few months her neck and upper part of her thorax were constantly turning crimson without any obvious cause, while the lower parts of the cheeks participated to a less extent. Paroxysms only persisted a short time and then passed off slowly. They were by no means as severe as in the previous case. Her mother had been for years a victim of Raynaud's disease. When the patient was examined the colour of her aura was uncommon, viz., green and blue not blended. The outer aura was wide and of average distinctness, ten inches by the head and twelve by the trunk. It had, however, an ill-defined margin, and gave the impression that an ultra-outer aura existed. A profile view showed the aura to be six inches in front, eight at the small of the back, and by the legs five, being slightly bow-shaped. The inner aura was plain and lineation obvious. The c.c. band exhibited three yellow patches on the back. The upper was small and situated over the third and fourth cervical vertebræ, the middle one over the second, third and fourth dorsal vertebræ, and lastly there was a large patch in the lumbar regions. In front there were two dark areas, one in either groin, separated from each other by an almost colourless interval. These two patches seemed raised about an inch from the body, and the aura between was massed. This was an unique phenomenon, as no other instance of this effect has ever been noticed, and the reason could not be determined. The three last patches were evidently due to ordinary functions, while for some undiscovered cause there was pain where the patch in the dorsal region existed. The most interesting point was the existence of the small spot on the nape of the neck, which occupied exactly the same position as did the one in the previous case.
A very remarkable case presented itself in September, 1916, and a second time a few months later. As certain points were of great interest and seemed likely
to furnish a key for the solution of several difficult problems, it will be fully described.
Case 79. P.B., a young Belgian woman of Flemish extraction, complained of deafness following on a relaxed throat. The uncovered part of her chest, which was triangular in shape was very conspicuous as it was of a deep crimson hue, far deeper than would result from mere exposure. In a few minutes it lost a good deal of its colour. After a remark upon its appearance she said that the slightest touch or rub on any part of her body would cause a red mark within a couple of minutes, which would last a considerable time. This had happened ever since she could recollect, and was accompanied by no abnormal sensations, so that she would be perfectly unconscious of the flush except for seeing it. Her skin was smooth and normal with no liability to rashes. She, as might be expected, bruised very easily. The mind did not seem to have any influence as an exciting cause.
When a nail was drawn lightly across any portion of the skin, a red line appeared on the part touched in from one to two minutes, a wheal formed and its colour gradually deepened to dark crimson. The blush spread upon each side of the wheal to the depth of half an inch or more according to the pressure used. This redness then declined slowly, leaving the wheal white. This would often persist half an hour or more. A slight flick of a pencil produced the same effect. A rub induced redness but the surface remained smooth. Every part of the body was similarly affected. Sensation on the wheals, as tested by the prick of a pin, was more acute than on the adjacent skin.
She was a small, well proportioned, very fair woman, twenty-two years of age, quick and intelligent and as far as could be ascertained did not evince any neurotic signs. Her health had always been good. She was the only child, and her parents were both alive and strong. Slight wounds did not bleed abnormally.
[paragraph continues] She believed herself to be more sensitive to tactile sensations than most women. Knee jerks were normal, and there was no abnormal response when the soles of the feet were tickled. The superficial reflexes were much exaggerated. With the sphygmometer a pressure of 118 mm. of mercury was required before the pulse was obliterated.
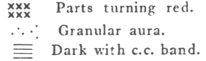
Both auras were of normal distinctness. The colour was peculiar—a whitish grey-blue mingled with a little green. The white imparted an opaque look, which was increased in the interspaces between the arms and the body, as the girl stood with her arms akimbo. As she faced the observer, the aura was nine inches round the head, the same by the sides of the trunk contracting to four by the feet. Seen sideways, it was four and a half inches in front, and the same width at the back by the shoulders and buttocks, coming down straight. This aura was perfect in shape and of average size for a woman. The inner aura was three inches over the whole body, with natural striation. The blue c.c. band disclosed a small purple patch, which was darker with the red band, on the neck from the third to the fifth cervical spines and nothing more.
After this preliminary investigation, various parts of her body were rubbed or lightly scratched, and the aura was examined during the time the changes were proceeding. As in each instance similar alterations took place, one description will suffice.
The central line of the body between the ensiform cartilage and the umbilicus was gently rubbed for a few seconds. For the first minute or so no change occurred, but gradually both auras seemed to widen, and become more distinct and opaque, and at the same time the etheric double, which was not noticeable before, became very clearly marked. It was half an inch in width. The outer aura soon enlarged to its maximum, which was eight inches, just twice its normal breadth. The inner aura when seen through
the red screen was about five inches broad, coarsely granular, and had completely lost its lineation. It had not the slightest resemblance to any ray. This condition lasted a few minutes, after which the auras gradually resumed their natural state, keeping pace with the fading of the red colour.
In the next experiment, with the hands resting on the hips and the elbows extended, the aura in the diamond-shaped spaces so formed with the body, was examined with screens before and after gentle friction had been applied to one side of the chest. The following were the results.
Up to the present time, with the exception of this patient, although the aura has been constantly examined for it, no local change has been detected over parts where redness has been induced by friction. This may, perhaps, be attributed to the fact that ordinarily only the most superficial layers of the skin are affected, while in the case above described the deeper layers ot the corium were probably also involved. It is more likely than not that even in a normal subject if the force used were sufficient to cause slight bruising, the aura would be influenced immediately or within a short time.
In another experiment the cervical spines were gently percussed with the finger in the region where the purple patch was seen with the c.c. band. It was not expected that this proceeding would have any influence upon the aura, but almost instantaneously
a general enlargement took place, yet not to the same extent as when static electricity had been used on a previous occasion. The width was eleven inches round the head, twelve by the trunk, and six by the feet, and when she stood sideways it was six by the shoulders continuing straight down the back.
This case differs from the last two inasmuch as the previous patients had only the upper part of their bodies affected. In them the skin frequently became red without any appreciable cause, while at other times the colour was induced by emotion, or some slight change in temperature, etc. The epidermis was deranged in the affected parts, which were dry, and in the worst places, even scaly. The urticarial reaction could always be produced over, and was wholly confined to, the abnormal areas. The colour changes, too, never attained the same depth as in the last instance, and only at the very darkest portion in the case 77 did they approach those usually induced by the slightest friction at any point in the affected area in the woman P.B.
It is certainly a curious coincident, if a coincident it be, and it hardly looks like one, that in all these three cases the c.c. band disclosed a coloured spot on the nape of the neck. In the last instance this was the only patch that could be detected over the whole of the body, with the exception of a very faint one on the sacrum. The presence of other patches over the different parts of the spine had been expected whether or not one occurred on the neck.
Case 80. E.D., a woman twenty-seven years of age, was inspected for the first time in 1913. She had been nursing her mother through a long illness, and immediately afterwards her father required great attention on account of his health. As a result she became greatly depressed and run down. For some months at intervals, her lips, both hands, and to a variable extent her forearms, became deeply cyanosed.
[paragraph continues] The attacks were sudden in onset, and often continued a considerable time. She experienced no pain but her hands were always cold. Although there was no heart disease, she suffered constantly from palpitations. Tache cerebrale could always be obtained on the chest and the back, almost as far down as the waist.
With the patient standing facing the observer, the outer aura was well marked, being seven inches by the head, eight by the trunk and three and a half by the ankles. A side view showed it to be three and a half inches in front, while at the small of the back it was seven inches, exhibiting a bow-shaped bulge, which commenced at the top of the head and finished at the feet. The colour was a blue-grey. The inner aura, as might be expected from the state of her health, was indistinct, nevertheless lineation was present, but was coarse in the lumbar regions. Three yellow patches were seen with the c.c. band on the back, the two lower being very plain but the upper not so definite. The highest one was situated on the third and fourth dorsal vertebræ, the central one over the twelfth dorsal and first lumbar, and the third over the sacrum. In front there were also three patches, all of a yellow colour with the blue c.c. band, and of a peculiar indescribable hue with the red band. The highest was over the epigastrium and left hypochondrium, the second was on the right side level with the umbilicus, and the lowest on the left groin. She had pain and tenderness in all these discoloured areas, especially the lowest on the back and the one in the groin during menstruation, at which time the pain was always severe. Indigestion accounted for the upper spot in front.
In February, 1915, after recovery, she was inspected a second time. Of late there had been no cyanosis of the hands, and no palpitations. The only trace of her former trouble was an occasional duskiness
of her lips, seen not once a week. The c.c. band showed two patches on the back precisely in the same positions as before, but the central one was missing. The upper one had grown faint, and the lowest continued quite plain. In front there was a pale yellow patch over the epigastrium, smaller and less conspicuous than it had been at the former examination, while the dark patch in the groin remained unaltered. The fading spots will probably soon disappear. (See page 257.)
When considering the shape of the aura in ill-health, it was remarked that in cases of hysteria, the outer aura takes a very characteristic form quite different to that seen in non-neurotic persons, while at the same time the inner retains its natural configuration. This statement is correct but does not go far enough, as subtle alterations also frequently occur in the inner aura, some of which can be detected only by the aid of the c.c. bands. In hysteria the number and size of these patches reach their highest, and are rarely equalled or exceeded in other diseases.
The following is an exceptional case which is almost phenomenal as regards the number of spots.
Case 81. (Figs. 62 and 63.) S., an unmarried largely built woman, thirty-six years of age, was, from her appearance, one of the last persons likely to be hysterical. She, however, had always been nervous, and a few years before had a breakdown after the death of her mother, but had recovered in a comparatively short time. In 1913, after returning from a holiday spent at the seaside, she began to complain of vague pains in different parts of her body which continually shifted from one place to another, and varied in intensity. She had slight mastitis which quickly got well. The upper part of the right thigh was also painful and continued so for a long period. Another time she had pain in the epigastrium with indigestion, and occasionally globus hystericus. On
a different occasion she complained of acute pain in the left shoulder and upper part of the left thorax. No satisfactory causes could be discovered for all these troubles.
At the end of the year her aura was inspected, and was found to be of a grey-blue colour. Both auras
Figs. 62 and 63.
Multiple patches.
reached the healthy standard of distinctness. The outer was a typical spatulate aura, eight inches round the head, nine and a half by the sides of the trunk, and four by the legs with the usual curve. In front it was six inches wide, which was broad considering
the breadth at the sides, and in the lumbar regions it was nine inches, as there was a big bulge commencing at the shoulders and terminating just beneath the nates, below which it was four inches wide. The inner aura was three and a half inches by the trunk, and about an inch narrower by the lower extremities. The whole of this aura was plainly lineated except where it was granular. This latter condition existed by the right side of the neck, thorax, and at the small of the back.
The c.c. band showed a large lemon coloured patch on the left side in front, from the shoulder to the nipple line, the inner margin corresponding to the median line of the body. It extended round to the back where the edge took the outline of the scapula. A continuation of the lower part of the patch in front was dark to the level of the ensiform cartilage. There was a deep yellow spot on the left groin, and another dark one on the right hypochondrium. The upper part of the right thigh was a pale yellow in front and round to the back. On the back there was a dark patch on the second and third, a yellow one on the sixth and seventh dorsal vertebræ, and a third one continuous with the last but dark and extending as low down as the second lumbar vertebra. Lastly there was a dark yellow area over the sacrum. Wherever the c.c. band exhibited discolouration the patient had either pain or tenderness at the time of inspection or shortly before.
The patient referred to in chapter vii (case 47) exhibited a good many patches, and this was only what might have been expected after the severe illness she had suffered from a few years previously. In front there was a light yellow spot a short distance beneath the right clavicle, another on the epigastrium, and a third darker yellow on the upper part of the right thigh below Poupart's ligament. On the back there was a yellow patch under the left scapula, a
second on the spine from the fourth to the tenth dorsal vertebræ, and lastly a large one over the sacrum.
There does not seem to be as great a tendency to the development of patches in males as in females, but occasionally one or more may be seen. In almost
Figs. 64 and 65.
Locomotor Ataxy.
every instance where a man has shown more than three discoloured areas, he has been the victim of a grave malady, which would among women have produced far more numerous patches. The following cases of locomotor ataxy exemplify this statement.
Case 82. (Figs. 64 and 65.) H., a man of fifty-four
years of age, contracted lues when he was twenty-two years old. Twelve years later locomotor ataxy was diagnosed, and since that time he has attended several different hospitals.
His unsteadiness when standing made it difficult to examine his aura. All the symptoms of his illness were those usually met with in that disease, so they hardly need description. His aura was inspected in 1914. The outer aura did not reach the good health standard of distinctness, and was grey in colour. It had nearly the size and shape commonly found in a man, being seven inches round the head, five by the trunk, and four by the legs, five in front of the trunk and four lower down, while at the back there was a bulge commencing a little above the head and terminating a short distance beneath the nates. The widest part was eight inches. The inner aura, as anticipated, was decidedly below the normal in clearness, and had a granular appearance by the right side of the trunk and at the small of the back. Its breadth was two and a half inches, and at the back in the lumbar regions was a trifle more pronounced.
Three discoloured places were brought to light by the c.c. band on the dorsum, first an ochre coloured patch on the upper two or three dorsal vertebræ, a light yellow one over the eighth to the twelfth dorsal, and a third over the sacrum, which was a dark yellow. In front there was a dark patch over the thorax, and a second dark yellow, on the right hypochondrium.
Case 83. (Figs. 66 and 67.) X., an inmate of St. Joseph's Home, sixty-two years of age, developed tabes dorsalis several years ago. At various times she had been an in-patient of four London hospitals, of most of them more than once. She was a thin miserable-looking woman, who from her worn appearance had been a great sufferer. She had all the customary symptoms of the disease in a more advanced stage than the last case. She experienced frequent
bouts of pain, often agonizing, and sometimes was compelled to keep her bed for days together. She was quite ataxic, but at times with help could walk a little.
Her outer aura, contrary to expectations, was perfectly normal in shape, showing nothing indicative
Figs. 66 and 67.
Locomotor Ataxy.
Dark with c.c. band according to shading.
of a nervous disease. The inner had an average width all over the body, although far less distinct than during health. It was granular a short distance above the crest of the ilium on the left side but nowhere else. It was only with the greatest difficulty that a faint striation could be anywhere detected,
With the c.c. band a long dark patch about two inches wide reaching from the fourth dorsal to the first lumbar vertebræ, and a second in the lumbar regions, was seen. In front there was a dark area over the epigastrium and another over the hypochondrium. The most noticeable feature was an uneven darkening over the whole of both thighs back and front. The colour of the band on the upper part of the left thigh, and the middle third of the right thigh was several shades deeper than over the rest of the limbs. The legs exhibited no discolouration. The depth of colour corresponded to the severity of the pain, which was more intense in some places than in others, and has been indicated in the diagrams.
Since diseases of the chest form a large proportion of cases seen in every day practice, it might have been expected that they would offer a good field for the study of the aura, but as a matter of fact they have assisted very slightly in the investigations, and conversely the aura does not afford much aid in their diagnosis. There are several reasons for this. A very important one is that when a patient is suffering from an acute illness, he would of a necessity have to remain in bed. It is obvious that besides the difficulty of a background and the arrangement of the light, etc., it would in most of these cases be inadvisable, if not absolutely improper, to trouble a patient in such a condition with an investigation which must be unavoidably prolonged and fatiguing, while in the present state of knowledge the benefits derived from it could only be problematic. Chronic cases, on the other hand, can be inspected with impunity, and show changes in the aura, but none that have much diagnostic value. Although the examination might be interesting, attention has been mainly devoted to other conditions thought more likely to give results of practical importance. However, a description of one or two examples will give a good idea of the changes likely to be found.
Case 84. T., a married woman forty-three years of age, complained once that when coughing she brought up some bright blood. According to her account it was quite a teaspoonful. Although a very careful examination of her lungs was made, the affected spot could not be ascertained. Two days later her aura was inspected prior to the usual examination by auscultation, etc. The aura had the proper size and shape for a woman of her age, and showed no abnormality until the c.c. band was employed across her chest. A light spot about the size of a florin, on the left side in the intercostal space, about an inch from the sternum, was immediately noticed. As soon as a stethoscope was placed over this spot, fine crepidations could be heard deep down, and the writer believes, rightly or wrongly, this to be the part of the lung from which the blood exuded. Even if he had not seen the pale patch in the c.c. band, he hardly thinks the physical signs would have escaped his notice. From subsequent experience he is certain that the band would have shown some alteration had it been employed directly after the hæmoptisis. This was the only part of the lung in which any disease could be discovered.
Of all chest complaints, the one par excellence in which changes of the aura could be of assistance, is incipient phthisis, but at present there is no distinctive case to bring forward, as in fact there has been only disappointment with those that have been examined. Of course, if bronchitis or emphysema be present, since the whole or the greater part of the lung is affected, it would be unreasonable to expect the detection of a small tubercular focus by some slight alteration in the aura which would inevitably be masked by the changes due to the more general disorders.
The next instance is a good example of the changes which take place in the aura during chronic phthisis.
Case 85. G., a lady twenty-seven years old, became consumptive in 1905, and progressed unfavourably for a long time. She had pleurisy on the left side in 1906, pneumothorax in the early months of 1909, and in the middle of that year the right lung became affected. During the whole of that time she was in Scotland, but to the surprise of all her friends she gradually improved in health. She was inspected in 1911. Her condition was exceedingly good considering the state of her lungs. The outer aura was found to be of medium width, being eight inches by the head, and the sides of the trunk, contracting to four inches by the ankles. It was symmetrical, but its texture was not as fine on the left, between the jaw and the crest of the ilium, as on the right. The inner aura was three inches in breadth on the right side and only two on the left of the trunk, but was alike in size and texture over both thighs and legs. Striation was very distinct on the whole of the right side, but on the left above the shoulder and by the trunk as far down as the crest of the ilium, the inner aura was either coarsely granular or roughly lineated. Lower down it was normal. The c.c. band was darker over the whole of the left side of the thorax, back and front, while below the costal cartilages and ribs was a dark patch reaching from the median line to the side as far as could be seen. The latter fault was evidently due to indigestion caused by the overfeeding which had been part of the patient's treatment. On the upper part of the right side of the chest was a dark patch over the diseased area in the lung. It was considered that the aura revealed that the patient had great vitality, but that the left lung was completely disorganized.
As volition is a high attribute of the brain, through which the aura as a whole can be influenced, it may be confidently asserted that every cerebral derangement will affect the aura in some way or another. Probably
such disturbances do produce some modifications of the whole aura, but the majority of the changes are of too refined a nature to be perceptible, and only the cruder ones can be detected. The coarse alterations that are recognizable may be so strange in appearance, that not even the most imaginative person would be likely to invent them. Who, for example, could have devised the hysterical aura? The more one contemplates this prodigy the more inexplicable it seems.
Among women the ovoid shape (fig. 11) of the aura is evidently the highest form, and the nearer it approximates to this figure the more perfect it is. As before mentioned, the main peculiarity of the hysterical aura lies in its being disproportionately wide by the sides of the trunk and in the lumbar regions of the back, when compared with its narrowness lower down.
It is not yet possible to follow the stages of alterations undergone by the aura during its transformation from the normal to the spatulate shape. At first the idea was that the development of the aura, which naturally occurs during the transitional period in girls, might have been arrested round the lower limbs. Although this theory seemed reasonable, it was shattered by the fact that spatulate auras are occasionally seen round children, and even more often round adult males. Another view which seems to embrace all known cases and therefore is more likely to be correct, is that a true increase of the outer aura by the sides of the trunk with little or no augmentation by the thighs and legs is present. This idea is supported by case 55, and also by the fact that all hysterical auras seen in males have been far wider than any ever met with round healthy men. The theory receives additional proof from the accompanying bulge of the aura at the back, which cannot be explained in any other way than by local increase.
It is useless to speculate in the present state of our knowledge why this peculiar configuration of the aura should occur amongst hysterical women. The practical question arises whether a normal aura ever becomes spatulate. It seems probable that this may occasionally happen. But intermediate forms are rare. Theoretically they might originate both during the evolution of the disease and during recovery.
When the aura is seen to be imperfectly spatulate, it is impossible to decide at a single sitting from its appearance alone, whether changes have reached their maximum or are progressive. Several further examinations must be made, and as yet the writer has never had the chance of obtaining them. Fortunately another method is available, viz., the artificial enlargement of the aura by static electricity. This agent often accentuates peculiarities which without its help are too ill-defined for accurate observation. Since the discovery of this property special attention has been paid to the subject.
The outer aura of the patient discussed in the appendix to chapter vii., was complex, and reasons were given why it was considered normal for that person. Its great width, it will be remembered, was thought to be due to a spatulate configuration rather than to the presence of an ultra-outer aura. The question was, however, definitely settled by electricity, as after the woman had been negatively charged, the haze at once assumed the true spatulate figure. This seems to be an example of an aura changing to the spatulate type, as owing to the low grade of bodily development, the woman's aura might reasonably be expected to have remained narrow.
In epilepsy a different variation of the aura is encountered. Here instead of the outer aura being alone or more particularly affected (as in hysteria), both auras seem to be correspondingly modified, being unilaterally contracted. No explanation of this
diminution can be offered, and it is still more incomprehensible why the left side should be the one usually influenced. Patient's friends have been asked, whether during the attack one side was more affected, or whether the head was turned to one side; as if the convulsions were more severe on the one side than the other, some light might be thrown upon the question. These interrogations did not produce any satisfactory answers, as with one or two exceptions all said that they were too much upset to notice. The mother of one girl said that the child had more spasms on the right side.
It is positively certain that the aura is influenced locally when there is a circumscribed disturbance of nerves, but whether the alteration is the direct outcome of the nerve disorder, as happens in the case of functional derangements of organs, or whether the change in the aura is secondary and dependent solely upon the actually affected organ, has not yet been decided. Probably each of these causes either alone or in combination with the other may be operative in various cases or at various times in the same case. One fact stands out prominently, viz., that a local disturbance influences the inner with greater frequency than the outer aura, but when the latter is affected the former rarely if ever escapes.
Neuralgia may be taken as an example of the manner in which the nervous system operates upon the aura. Case 49 is a very good instance. When seen in 1909, it was noticed that the whole of the inner aura adjacent to the painful spot was altered, as all striation had disappeared and it had become granular in aspect. The outer, too, showed signs of disorder, as the distal portions were less plainly visible than usual, appearing less dense. In other words, the outer auric force was not so potent as when in health, but at the same time retained its general characters. Had the force been still further reduced, the haze would have contracted.
[paragraph continues] This was the condition of the aura when seen in 1908 (vide page 200), and it is evident that at the latter date the auric force was regaining its natural energy.
In an acute case of neuralgia, a girl thirteen years of age, had a spot at the level of, and two inches to the right of the third dorsal vertebra, where paroxysms of pain came on suddenly and often lasted for hours. The most common time for its accession was at night shortly before going to bed, or else soon after, but anyhow the spasm prevented sleep. There was no tenderness over the place, and no cause could be found for the trouble. The ailment was very intractable for some weeks, and then slightly improved. She developed appendicitis, when pain suddenly vanished and never returned. Her aura was examined and seen to be quite natural all over the body, with the exception of a small spot just above the painful place where it was granular. It was only in the inner aura that any change could be discovered. As the disordered patch must have been small, it is unlikely that the outer would exhibit any alteration since the surrounding healthy portion must certainly have acted as a mask. In this instance the c.c. band showed a dark spot, while in the previous case the affected aura induced a light shade.
Two or three patients suffering from sciatica have exhibited very similar changes in the aura down the whole of the affected limb. When a local organic alteration of tissue is dependent upon nervous derangement, it is probable that the modification that takes place in the adjacent aura is partially due to the nervous element, and in part to the diseased tissue, but it is next to impossible to decide the proportion associated with each factor. Herpes Zoster is a very good example of the combined causes, but so much has been said about these alterations that the reader is referred to the cases 57 and 62.
As these cases demonstrate that the nervous system
can induce transformations of the aura, both with and without a corresponding change in the local tissues, it might possibly be thought that the modification would be entirely dependent upon the influence of the nervous system, and that the disordered tissues had no share in its production. The only method of disproving this hypothesis is to find a case where the change in the aura cannot be credited to the nervous system. Fortunately notes were made upon several cases in which it is extremely unlikely that any deranged nervous agency could be present. The patients had superficial tumours, and the examples chosen for illustration are a fibro-adenoid, a cystic tumour of the breast, a fatty one of the thigh, and an osteo-sarcoma of the arm. In none of these cases could any alteration of the outer aura be discovered, but in each there was a derangement of the inner.
The fibro-adenoid caused the inner aura to assume the appearance of a small ray, not more than one and a half inches in length, slightly wider than the breadth of the aura, and granular. When viewed with the blue c.c. band, it was seen as a spot lighter than the rest of the band, and with the yellow, darker.
The cystic tumour gave a somewhat similar effect, except that the inner aura was altered throughout its whole width, the change consisting of a coarse granular condition replacing the ordinary striation just over the tumour. Examination of this ray by the aid of the c.c. bands, showed a light area with the blue and a dark one with the yellow.
The fatty tumour was a moderately large one of several years standing, on the outside of the left thigh of an otherwise healthy woman, thirty-six years of age. Inspection did not show any perceptible change near the growth until the c.c. bands were employed. With each of these bands the haze over the tumour looked lighter than the rest of the band, indicating that some delicate modification had taken place.
The last example was an osteo-sarcoma of the humerus. Here the aura assumed the appearance of a coarsely granular ray without any signs of lineation. The blue c.c. band produced a discoloured spot of a most unusual colour, which can only be designated by pinkish-yellow.
From the above remarks it may be taken for granted, that although the nervous system has a very great, perhaps a predominant control over the auras, yet other tissues when in an unhealthy state do influence them as well. In this connection it will be interesting to compare case 72 with case 76. In the former the patient had an ulcer of the stomach which caused the c.c. band in front to be lighter than the natural hue of the band. The inner was also granular in the gastric region. It must be noticed that there was no change in colour of the band near the dorsal vertebræ. In the latter, although the woman was suffering from constant vomiting, there was only slight granulation in the gastric region, and the c.c. band did not disclose any alteration of colour on the front of the body, but on the back there was a narrow streak lying close to the spinal column on the left side, from the third to the fourth dorsal vertebræ, decidedly lighter in colour than the rest of the band, and with sharply defined margins. In the former of these examples, it looked as if the diseased organ was the factor producing the alterations, while in the latter the stomach only influenced the aura slightly, but the main change in the band was due to a nervous element.
Enough has been said in this chapter to show how important a part the c.c. bands play in investigations, and how great is the assistance they can give in diagnosis, both positively and negatively—positively, by demonstrating that the auras have undergone some alteration locally, the result of a disturbance at that place, and negatively, by proving that no appreciable
change has taken place where an underlying disorder has been suspected. It is, however, necessary to remember that the c.c. band may occasionally not show alteration when it is known that the part beneath it is diseased. The help that this band can give is thus limited, but becomes greater and greater as the observer gains experience by practice in appreciating the finer differences manifested. The mischief in instances giving negative results is, almost without exception, of slow progress, such as takes place in contracted kidney, while the more acute and active changes will be more likely to induce alterations in the auras, and consequently in the c.c. bands.